


As Part of the Cast Off 22 Program Vet Info has established Fishing Fridays at U.S. Southern Command. This will be an on going program over the next 12 months to give the Active Duty and Veterans who work at the Installation a chance to learn how to fish or increase their skills with Bass Pro Shops Pro Bill Watts and the Vet Info Volunteers.
















































Vet Info to speak at the City of Doral to enhance it Programs within the City and create a partnership with the city.
Today we celebrate the sacrifices made by Veterans. But do we really understand the sacrifice? Can it really be summed up in one day of remembrance?
How do we console the family members who do not get to see their beloved Veterans anymore? How do we make up for missed births, birthdays, dance recitals, swimming competitions, school debates, anniversaries, and so much more? What about the first steps or first words of a baby? How do we only remember for one day that we are losing more than 22 veterans per day? How do we count the days of a soldier who has not been found or returned home?

Can we really celebrate for one day the daily pain many Veterans face due to their unwavering service to our country? Agent Orange and burn pit side effects, lost limbs, and mental health does not rest for 364 days until the next Veteran’s Day.
As we honor our Veteran heroes, we must not honor them for only one day. We must honor the never-ending pain and struggles they confront daily.
No Veteran Left Behind, Conflict, Does Not End on the Battlefield!
Vet info is honored to receive a $2000 grant from Bass Pro. The funds will be used to further our cause of improving the quality of life of military veterans.
Bass Pro has been instrumental in our success and ability to serve the Military Veteran community. We are a grassroots organization with no employees. Support from Bass Pro and other organizations who want to serve military is truly inspiring and appreciated.
In 2022, Bass Pro Miami, Tampa, and Ft. Myers help us with providing t-shirts for Veterans living in retirement homes. We provided over 400 gift packages that included shirts, puzzle books, hygiene supplies, and a holiday card written by high school students.


One of Vet Info’s programs is kayaking. Sometimes we fish too. Bass Pro helped us with the purchase of the Kayaks. We are very grateful for the two Old Towne PDL 120s and the four Ascend 12ts. This photo was taken at the Miami Lakes Veteran’s Day Parade 2023.
The Veteran below never thought he could ever go and kayak. He suffers from many issues onset from Agent Orange when he served as a Marine in Vietnam. He found kayaking to be fun and easy to do and has even thought of buying his own kayak.

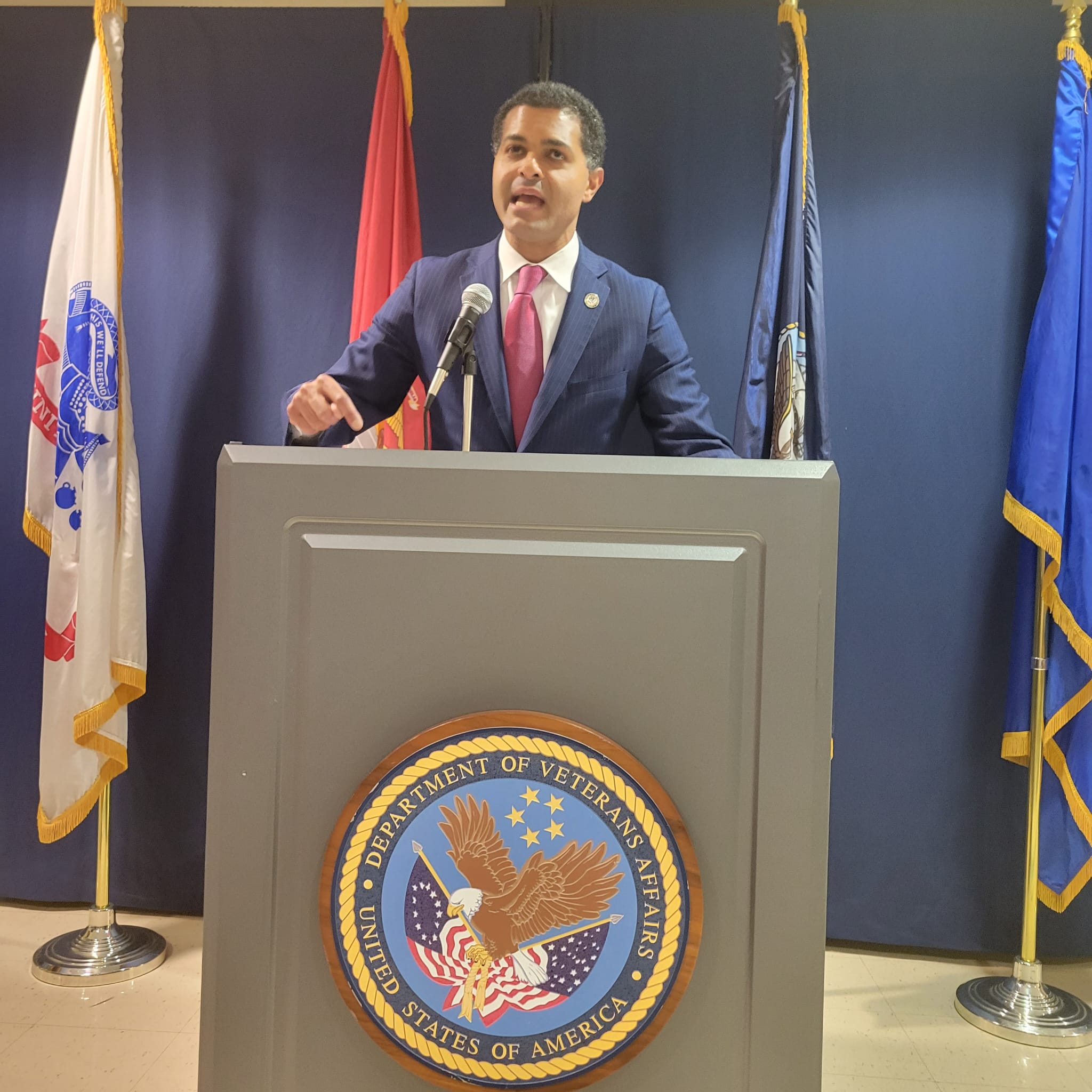
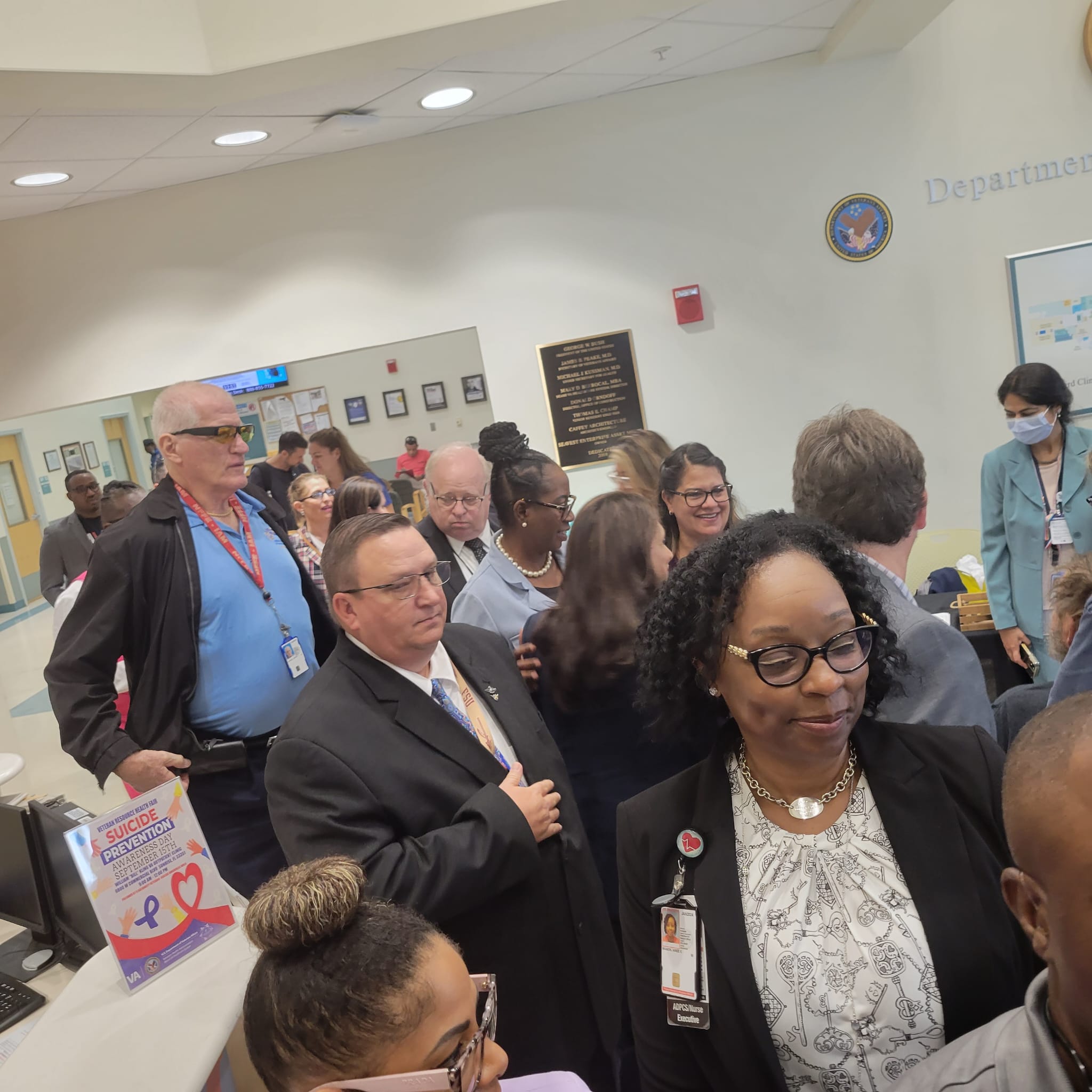
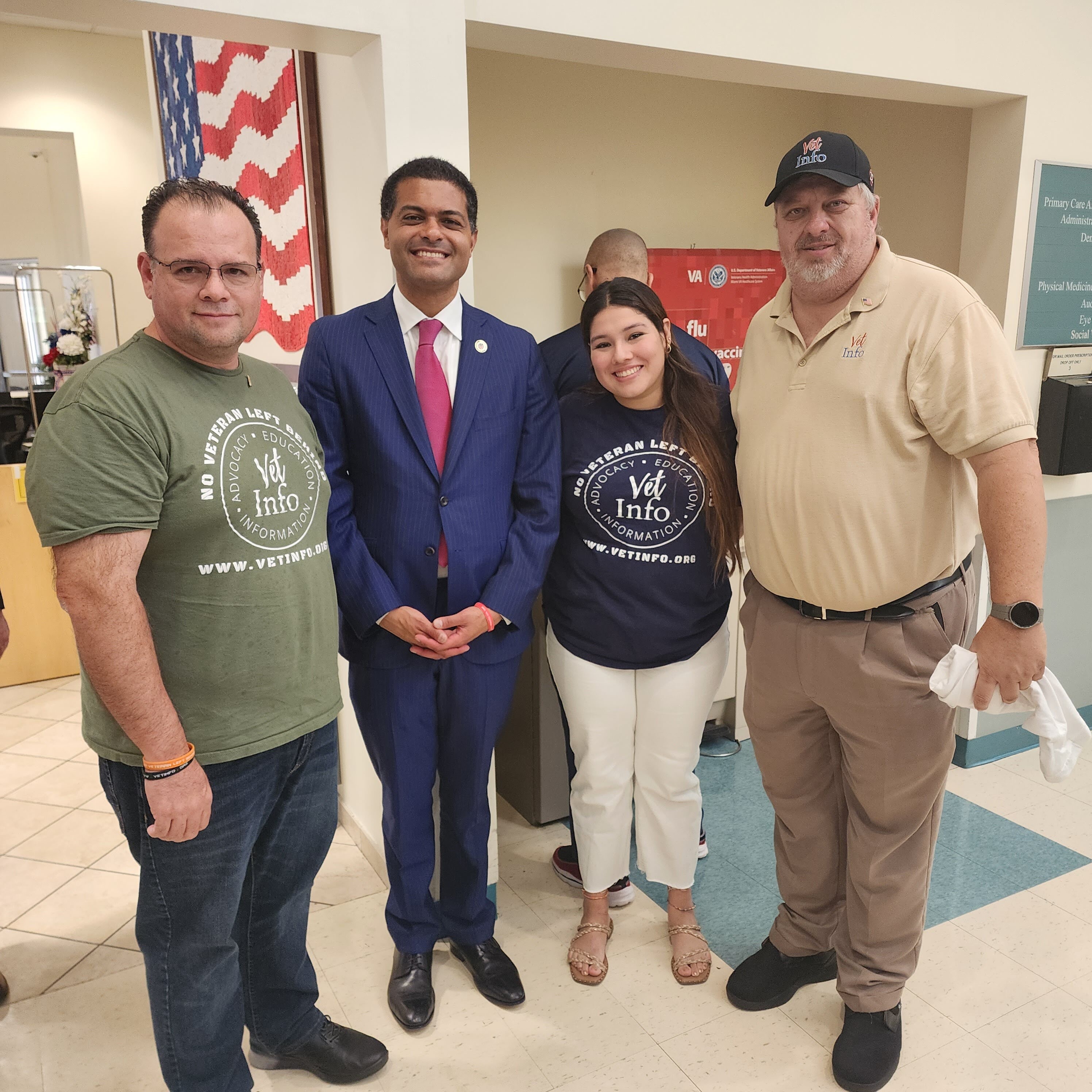
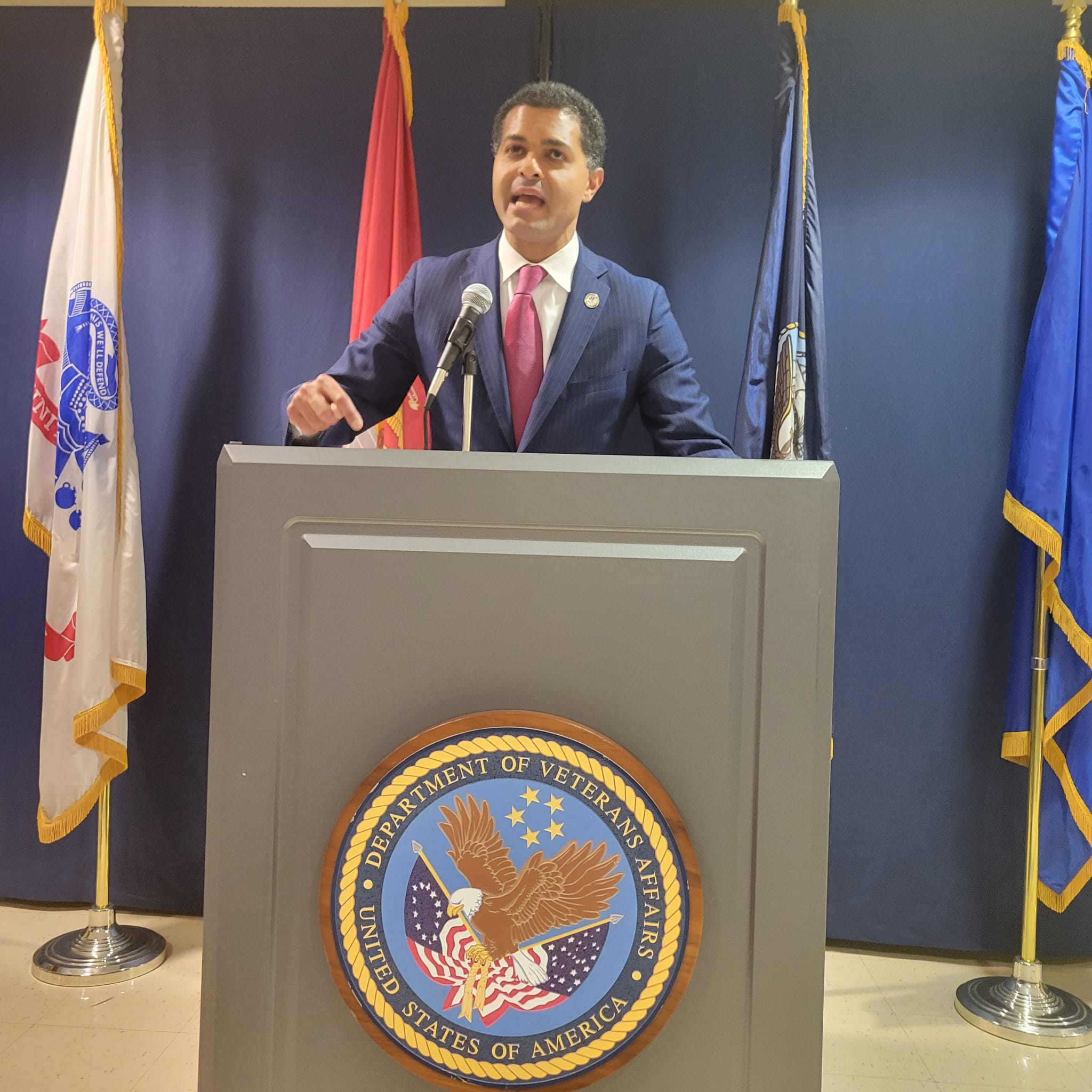
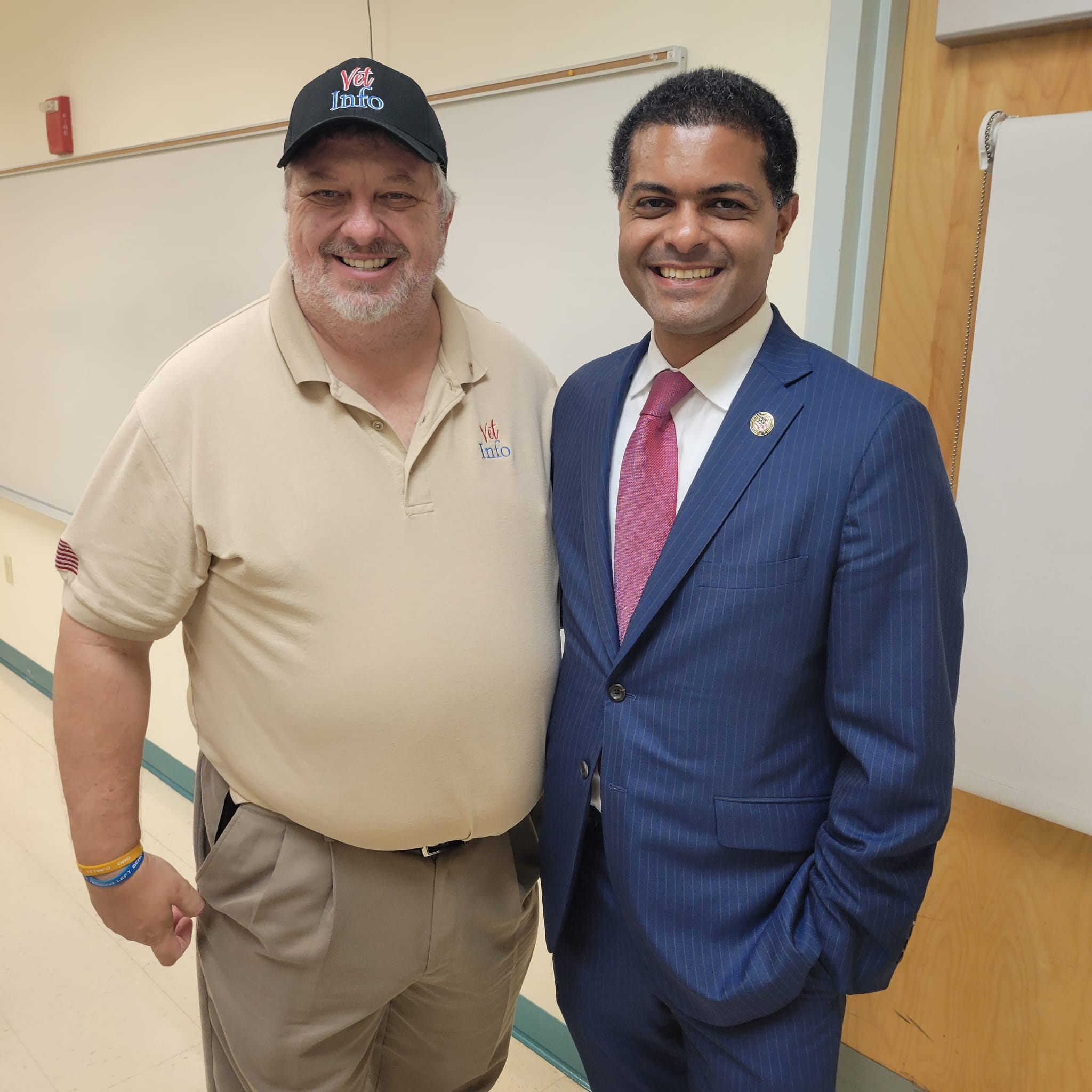
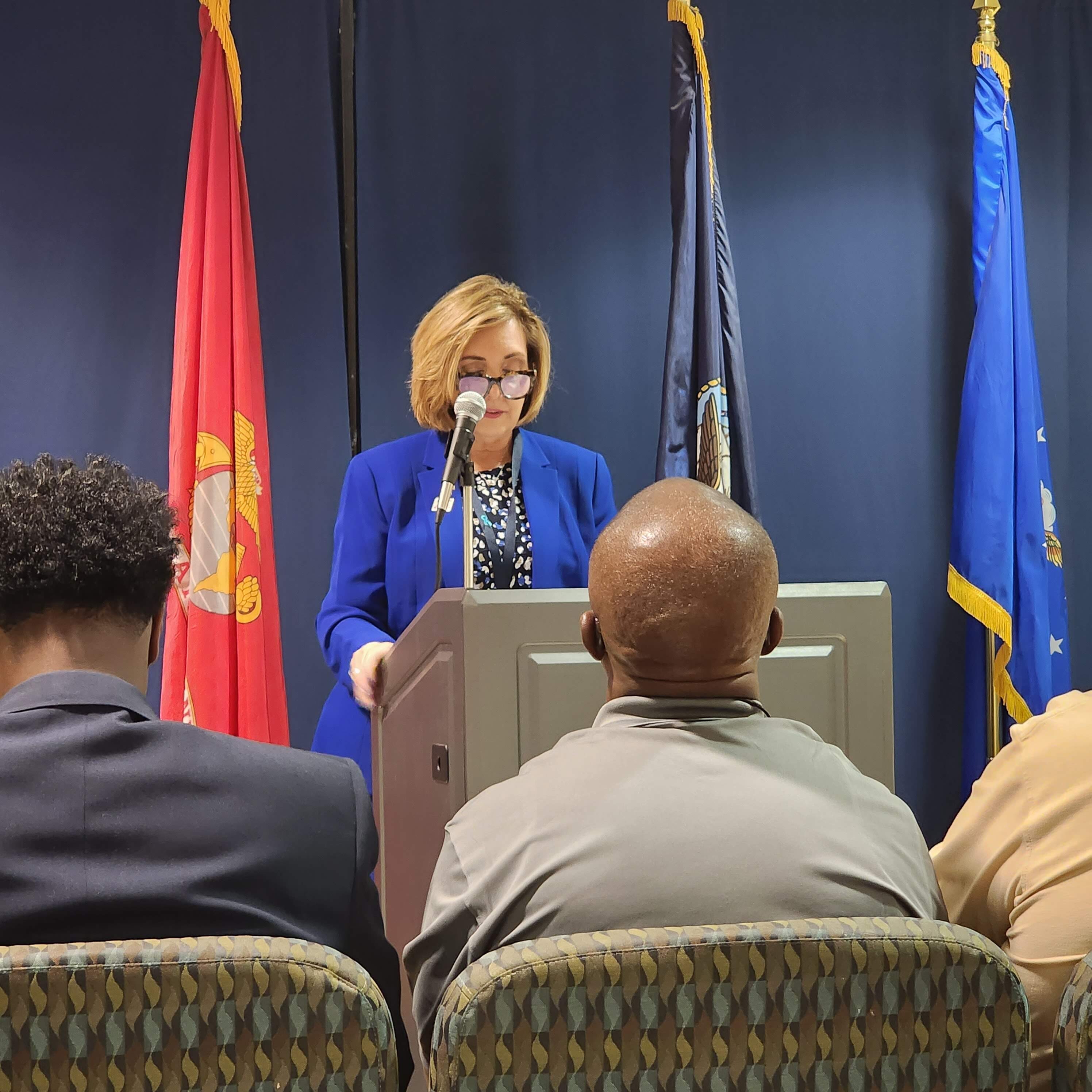
Vet Info participated in the Suicide Awareness Month event at the William “Bill” Kling Community Outpatient Clinic with the Miami VA. Many community organizations/non-profits participated to share how we all support our hero military veterans. Dr. Shereef Elnahal, Under Secretary for Health at the Department of Veterans Affairs spoke at the event and conveyed the importance of the need for the community and the VA to unite and combat the epidemic of suicides amongst veterans.
Dr. Elnahal, Under Secretary for Health at the Department of Veteran Affairs was kind enough to give us a plug about our bracelet at 2:36. “No Veteran Left Behind”





































On the 24th of August 2023 the City of Doral Florida celebrated its 20th Birthday. Vet Info Founder Bill Watts was one of the Honored for his contributions in helping Doral move from being an Unincorporated area in Miami Dade County to a City where you can Live, Work, Play and Learn.
































For years I have been a victim of being overweight and each visit to my Primary Care Provider (PCP) and the MOVE Clinic of the VA Healthcare system they always tell me I need to lose weight and provide me with information to look at a better way to eat. So in this post I am providing you with information on Carbs and and Gluten-Free Nutrition Therapy. This gives you great examples of low carb foods and foods to avoid. I hope you find this information helpful. Until next time your friendly neighborhood Capt. Bill